Part 1: medical documentation (MD)
DMP participants are meant to visit their diabetologist four times a year. The main events and parameters are discussed between physician and patient, recorded and sent to one of the 6 data authorities for testing and pseudonymisation.
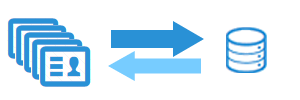
Data acquisition in a physician's practice
Pseudonymisation and forwarding
Data processing by MNC
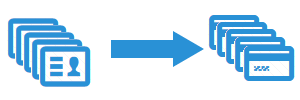
Part 2: data on patient characteristics (PM)
Data on patient characteristics is generated and transferred by the statutory health insurance companies. For each participant, information regarding their enrollment in a DMP, gender and age are transmitted.
Generating the data on patient chracteristics
Data transfer to Medical Netcare
Data processing by Medical Netcare
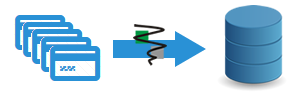
Part 3: Data for consolidating pseudonyms to a master record (MK)
The data for consolidating pseudonyms to a master record is generated and transmitted by the health insurance funds. The data consolidation program was established in order to pseudonymise all patients in a standardised way and is based on this data. Data on medical parameters and patient characteristics can deviate from the proper main pseudonym. For all records of one patient to bear the same pseudonym, pseudonyms are translated by the procedure depicted here into the main pseudonym.

Generating translation lists
Data transfer to Medical Netcare

Data processing by Medical Netcare
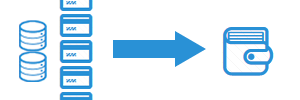
Part 4: Data assigning membership of a distinct health insurance fund (IK)
The institution codes (IK) used in the medical documentation can differ from the main institution code of a fund due to administrative reasons. In order to state a participant's membership of a distinct health insurance fund, these differing codes have to be translated. This is the only way to reunite medical documentations with patient characteristics. Institution codes are generated and transmitted by the health insurance funds.
Generating the institution code translation table
Data transfer to Medical Netcare
Data processing by Medical Netcare
Translation of institution codes
The new data is not yet containing the final health insurance fund's assignment. The included institution codes have to be translated first. By translating using the institution code translation tables, data is assigned to the correct health insurance fund.
Translating is processed for each of the three other data types: patient characteristics, medical documentations and consolidation data.
In case of modifications in the translation tables, all records in stock are to be translated by means of these new tables. For example, this case occurs when two health insurance funds fuse. The institution codes of the fusioning funds are joined via new translation tables. This way, such modifications are implemented rather quickly.

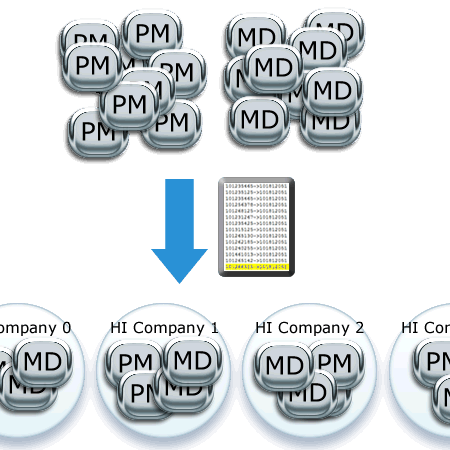
Generating master records - translating pseudonyms
The translation lists by the health insurance funds are provided twice a year. Each time they arrive at Medical Netcare, the whole stock in translation rules is replaced and rebuilt. This means, on the one hand, that the translation is to be operated on the whole data in stock – on the other hand, a health insurance fund can report tranlations late or correct them providing missing data to connect medical documentations to the respective patient characteristics in retrospect.
The translation is operated on the patient characteristics provided by the health insurance funds as well as on the medical documentation.
When the translation is processed, the data fusion is complete for the moment. Now, MNC checks for loose ends (medical documentation without matching patient characteristic record or vice versa) and reports these to further enhance data quality. Within a time limit of 4 weeks, MNC accepts corrections or additional data. Afterwards, the data processing is finished.
Progress documentation
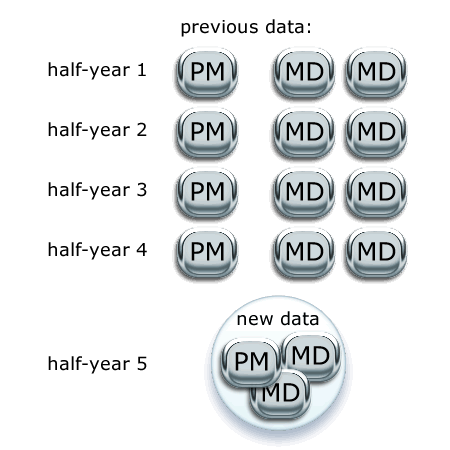
In their translated form, all data of a patient can be merged sensibly. The data of each DMP participant is a progress documentation by now.
The diagram on the left depicts a patient's progress with respect to the data. In order to further procede the data, a few more steps and algorithms are necessary. The current evaluation demands analyses on the basis of half-years as well as years. Due to regular consultations , there are normally two medical documentations per half-year (and accordingly four in a year). For example, each patient has two blood pressure values and two HbA1c values in a half-year. Data has to be further concentrated to suit the systematic evaluation with just one value per observation time.
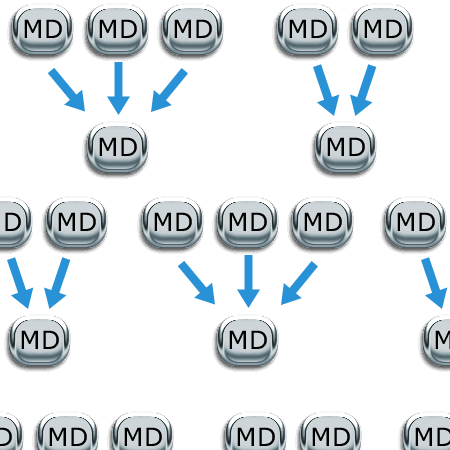
Operationalisations to condense data
Within DMP evaluation, yearly as well as half-yearly presentations are chosen for the evalution of data. If there is more than one medical documentation per patient and evaluation point, documentations have to be condensed.
MNC developed operationalisations prescribing for each medical parameter how to calculate or determine them. In defining these operationalisations, we took care to understand the meaning of each value and condense them accordingly. These are a few representative rules:
- the value from the first or the last documentation in an evaluational (half-)year is adopted
- the major or minor value out of all available documentations is adopted
- the value transporting the worst or the best statement is adopted
- the arithmetic means or a sum is built on the basis of all available documentations
Report production
The requested evaluations for DMP are only possible with the data preparation being processed.
new reports are produced per indication.
These additional regulations are taken into account for the production of reports:
1. The year of the first publication of an to the DMP-A-RL is the last year to be included in the first report following the new systematic. Afterwards, sentence 3 applies.
2. The report has to be handed in no later than 18 months after the year of the first publication of the annex ended. Afterwards, sentence 3 applies.
3. The interval between indication-specific evaluation reports is three years.